One of the hardest things to achieve in cases of TSL is to find the main cause of the problem. There are four categories of TSL - erosion, attrition, abrasion and abfraction. However, more often that not once one type of TSL starts others will play a contributing role. However most of the time there is a primary or initial cause. Once, this main cause is identified then the most appropriate preventative advice can be given and the most effective treatment recommended.
Erosion
Erosion is by far the most common type of TSL we see. It can be very rapid and occur at a young age. It is caused by the repeated exposure of dental tooth structure to acid - most commonly dietary but also, whilst less common and far more damaging, stomach acid.
Dietary acid is the main cause due to huge increase in the consumption of acidic foods and drinks.
Dietary acid is the main cause due to huge increase in the consumption of acidic foods and drinks.
- Soft drinks and fruit juice consumption has doubled since 1970 and gone up by 700% since 1950.
- 65% of sales are by adolescents and children.
- 42% of fruit juice is consumed by 2-9 year olds.
- Over 50% of drinks sold are diet & carbonated many with a pH <3.
- Alcohol consumption is increasing especially acidic drinks ‘Alcopops’ & wine

Historically the main cause of erosion was attributed to carbonated ' fizzy' drinks. However the current research shows that fizzy drinks actually place a smaller role than previously thought. This is because even though the ph of the drinks is very low they are almost immediately buffered once swallowed and the oral ph rises almost immediately after consumption. They will still play a role when consumed in excess as shown by the middle picture below - a 34 year old man with a habit of drinking 3 litres of diet cola and dry cider per day.



The greater cause of erosion is due to the frequent eating and chewing of acidic fruit. Patients who consume several pieces of fruit a day or drink 'juiced' drinks made with fruit are more at risk of erosion. The evidence above shows the consumption of acidic fruit and fruit juice has risen, especially in children. Also the consumption of energy drinks has been shown to be a rising cause in dental erosion.




|
Stomach acid can also play a large role in dental erosion. Even though it may be less frequent the effects of stomach acid contacting the dental tissues can be very damaging.
There are the well known eating disorders anorexia nervosa and bullimia. These can be very serious conditions and difficult to treat. However, more commonly stomach acid is coming into play involuntarily. Acid reflux is very more common a cause. Obesity levels are rising causing gastric regurgitation, usually whilst lying down at night and very often asymptomatically. More patients are being treated for heartburn and are on medications to neutralize the acid such as antacids, or reducing the production of acid. Therefore, when erosion is seen care should be taken to obtain a full diet history with particular care in finding high, frequent consumption of acid fruits, fruit juices and energy drinks throughout the day. A complete medical history taken with questioning over any symptoms of acid reflux is essential. We will discuss the aetiology of erosion in more detail in a later blog. |
Attrition

|
Attrition is the type of TSL that is a result of tooth to tooth contact. The tooth loss will be limited to the occlusal surfaces of posterior teeth and the incisal and palatal surfaces of the anterior teeth that are in contact during the chewing or parafunction.
The surfaces affected tend to have straight, flat and smooth surfaces as shown in the picture on the left. However, once dentine is exposed then it will wear more quickly and create areas that are ' dished out'. This is because the dentine is much softer than the surrounding enamel and erosion will start to play a role in the TSL due to the exposure to acid. |
We expect to see a small amount of attrition as part of the normal aging process. However, during normal mastication, this is in the region of 10 microns a year so will not be the cause of majority of the excessive attrition we will see. There are normally three main causes of attrition we will see.
1. Firstly, teeth exposed to excessive occlusal forces due to the slow reduction of their OVD - as shown in the picture above. Or as a result on the loss of a stable posterior occlusion through loss of the posterior teeth. The remaining teeth take excessive occlusal forces and suffer attrition as a result.
2. Secondly, teeth exposed to repeated, high occlusal forces as a result of parafunction or 'grinding'. However the teeth can be in a stable, healthy occlusal scheme. This can be caused by night time grinding or the picture below on the left shows a patient with flat attrition on his posterior teeth as a result of the parafunction caused by years of ecstasy use in clubs! In habits like this and parafunction the attrition affects surfaces exposed to right/left jaw movements and will be limited to the posterior occlusal surfaces and possible the tips of the anterior teeth. There does not tend to be any attrition on the occlusal contacts seen in normal functional chewing.
1. Firstly, teeth exposed to excessive occlusal forces due to the slow reduction of their OVD - as shown in the picture above. Or as a result on the loss of a stable posterior occlusion through loss of the posterior teeth. The remaining teeth take excessive occlusal forces and suffer attrition as a result.
2. Secondly, teeth exposed to repeated, high occlusal forces as a result of parafunction or 'grinding'. However the teeth can be in a stable, healthy occlusal scheme. This can be caused by night time grinding or the picture below on the left shows a patient with flat attrition on his posterior teeth as a result of the parafunction caused by years of ecstasy use in clubs! In habits like this and parafunction the attrition affects surfaces exposed to right/left jaw movements and will be limited to the posterior occlusal surfaces and possible the tips of the anterior teeth. There does not tend to be any attrition on the occlusal contacts seen in normal functional chewing.

|
|
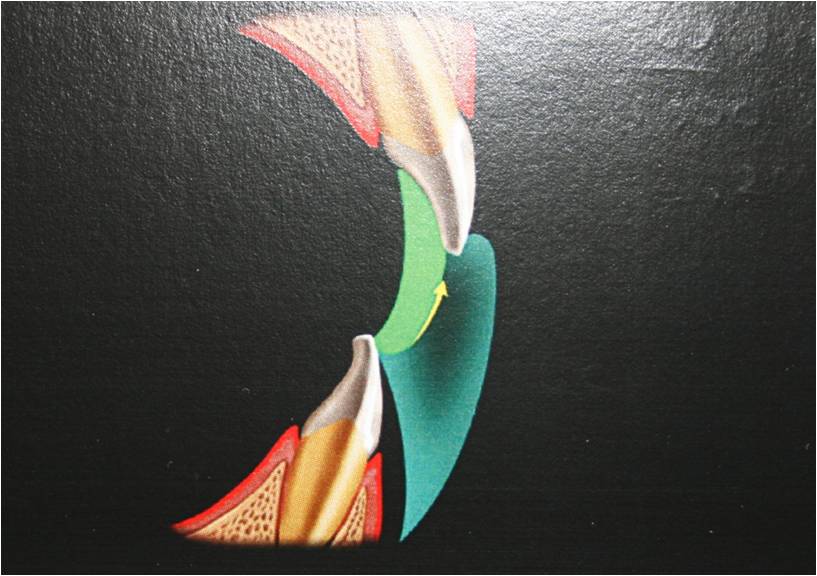
3.The last, and most common type of attrition will be caused by normal chewing but where the teeth are not in a stable occlusal scheme. The picture on the right, above, shows the normal cycle of chewing and the anterior teeth 'guiding' the posterior teeth into a stable, reproduceable intercuspal position (ICP). There is either a problem with the posterior teeth - dysfunction, or the anterior teeth position - constricted chewing pattern.



Dysfunction - this is where there is not a stable posterior ICP for the patient's posterior teeth to sit in at the end of the chewing cycle. Therefore, the patient has to posture their mandible so that it can find some position where the posterior teeth will contact. This will cause the normal envelope of chewing to be altered, as seen in the picture above on the left. This will result in teeth coming into contact during chewing and resulting in tooth loss from attrition due to the chewing forces. The pictures above on the right show a lady with the ICP that has adapted and been created as a result of having to posture the mandible to the left to 'find' a working ICP. This is because there is not a stable posterior occlusion that the patient can find as a result of the overerupted upper right wisdom tooth and the edge to edge contact of the left canines due to the discrepancy is arch sizes on the left. The ICP that has been postured into in the middle photo has resulted in attrition of the anterior teeth as a result. Dysfunction will usually result in attrition that flattens the cusp tips or incisal edges.
A constricted chewing pattern is caused by the upper anterior teeth being positioned within the normal path of the lower jaw during chewing. This can be seen in the diagram in the middle, below. There is a stable, reproduceable posterior occlusion or ICP that the patient can find at the end of the chewing cycle. This situation can be created as a result of orthodontic treatment, prosthetic replacement of the front teeth with fixed or removeable prostheses or during normal development. Having upper anterior teeth in this position means that they are going to be exposed to high occlusal contacts during normal chewing cycles. However, this will not always result in TSL as the patient can learn to retrude their mandible slightly during chewing in order for the lower incisors to miss the upper palatal surfaces. However, over time this can result in attrition that affects only the surfaces on the front teeth between the initial contact during chewing and the final position found once the posterior teeth meet in ICP. This can be seen in the photo below on the right. The initial contact at the inicisal edge with the occlusal contacts all the way down the palatal surfaces until the teeth meet in ICP - this will create a classical ridge or notch seen on the palatal surface.
A constricted chewing pattern if present or created in a patient who also has or develops a high acid intake can result in very rapid TSL. This will affect the palatal surfaces and will result in the thinning and translucent appearance of the anterior teeth as shown in the photo on the left below.
We will discuss the treatment of these different situations in a later blog. If you would like to learn more on the management of the occlusion then I would strongly recommend the Kois centre in Seattle that has a fantastic course on occlusion and who created the three diagrams seen in this section.
A constricted chewing pattern is caused by the upper anterior teeth being positioned within the normal path of the lower jaw during chewing. This can be seen in the diagram in the middle, below. There is a stable, reproduceable posterior occlusion or ICP that the patient can find at the end of the chewing cycle. This situation can be created as a result of orthodontic treatment, prosthetic replacement of the front teeth with fixed or removeable prostheses or during normal development. Having upper anterior teeth in this position means that they are going to be exposed to high occlusal contacts during normal chewing cycles. However, this will not always result in TSL as the patient can learn to retrude their mandible slightly during chewing in order for the lower incisors to miss the upper palatal surfaces. However, over time this can result in attrition that affects only the surfaces on the front teeth between the initial contact during chewing and the final position found once the posterior teeth meet in ICP. This can be seen in the photo below on the right. The initial contact at the inicisal edge with the occlusal contacts all the way down the palatal surfaces until the teeth meet in ICP - this will create a classical ridge or notch seen on the palatal surface.
A constricted chewing pattern if present or created in a patient who also has or develops a high acid intake can result in very rapid TSL. This will affect the palatal surfaces and will result in the thinning and translucent appearance of the anterior teeth as shown in the photo on the left below.
We will discuss the treatment of these different situations in a later blog. If you would like to learn more on the management of the occlusion then I would strongly recommend the Kois centre in Seattle that has a fantastic course on occlusion and who created the three diagrams seen in this section.



Abrasion
The loss by wear of tooth substance or a restoration caused by factors other than tooth contact. This can be caused by long term habits - such as the notches formed on the front teeth after long term pipe smoking or playing a musical instrument with a reed. More stranger causes are electricians who habitually stripped the insulation off wires with their teeth or keen sewers who hold needles between their front teeth. However, all these are going to be quite rare and once the offending cause eliminated quite easy to restore.

|
The more common cause was thought to be excessive toohbrushing. However, the resent research would indicate that this is not quite true. Excessive toothbrushing across the necks of the teeth can result in recession and exposure of the root. This can result in sensitivity. However, the physical brushing of the bristles has been shown not to result in the removal of tooth tissue and the creation of lesions such as those shown on the left UNTIL ............... the introduction of an abrasive toothpaste.
The Relative Dentine Abrasivity score of all toothpastes is not widely advertised but is easily found through a google search. The more abrasive the toothpaste the more likely it is to help remove tooth structure of an exposed soft root surface. The main issue is that many more of our patients are using whitening toothpastes for cosmetic reasons and these all tend to have a higher RDA value. |
However, as usual tooth surface loss caused by abrasion will usually have several risks factors working together before tooth structure is lost. The brushing habits will probably be too hard, the toothpaste being used slightly too abrasive and the exposed root further softened due the frequent exposed of acid. Therefore, the prevention of these types of lesions will need to consider the elimination of all these factors.
Abfraction.
This is the most controversial type of TSL with clinicians either believing that this condition exists or not. As can be seen in the pictures below the theory outlines the slow breaking of the enamel prisms at the point the enamel is the thinnest - at the crown/root interface. Excessive occlusal forces, particularly in lateral guidance, result in the slow formation of a class V cavity at the neck of the tooth.

|
I personally do believe that this theory has some merit for several reasons. 1. These lesions are usually seen on the premolars, as shown left. If other causes such as hard or excessive toothpaste/ tooth brushing use were to be the cause how has the canine remained untouched? Such habits would apply far more heavily on the exposed canine root than the premolar root hidden behind and slightly instanding. 2. Very often the base of the lesion is below the level of the gingival margin. Again if toothbrushing is thought to be the cause how has the hard tooth structure been removed leaving the very much softer gingival tissues intact overlying the lesion? This can be seen in the picture on the left. 3. When I see these lesions there is always a heavy functional occlusion, not in ICP, but in lateral guidance or the functional chewing pathway. This is either developed as part of the current occlusal scheme or the heavy contact has slowly been created as the existing canine guidance is lost. The canine itself is worn through another TSL process - such as attrition in the pictures on the left. Therefore, it is very important when you see lesions such as these that you fully assess the current functional occlusal scheme. |




However, I do believe that the creation of an actual lesion cannot be completely contributed to just one single cause and I feel several factors need to be working together to result in the creation of a class v lesion. The presence of a heavy functional contact on the cusp alone may not always result in an abfraction lesion, however a lesion may develop in a patient who also has repeated acid attacks - such as regular consumption of acidic fruits and who may brush with a slightly abrasive toothpaste. Hence, for a class v abfraction lesion to develop there needs to be several risk factors of TSL and an unfavourable occlusion all working together.
Let me know what you think and we can start the debate !!!!!
Let me know what you think and we can start the debate !!!!!